+91-7056170571
paramedicalskilldevelopment@gmail.com
Home
About Us
About Us
Vision And Mission
Franchise
Franchise Registration
Registered Franchise
Courses
Healthcare
10th /12th
10th
12th
PARAMEDICAL
10th
AFTER 10 TH
Electrocardiography Technician
Download
Migration Form
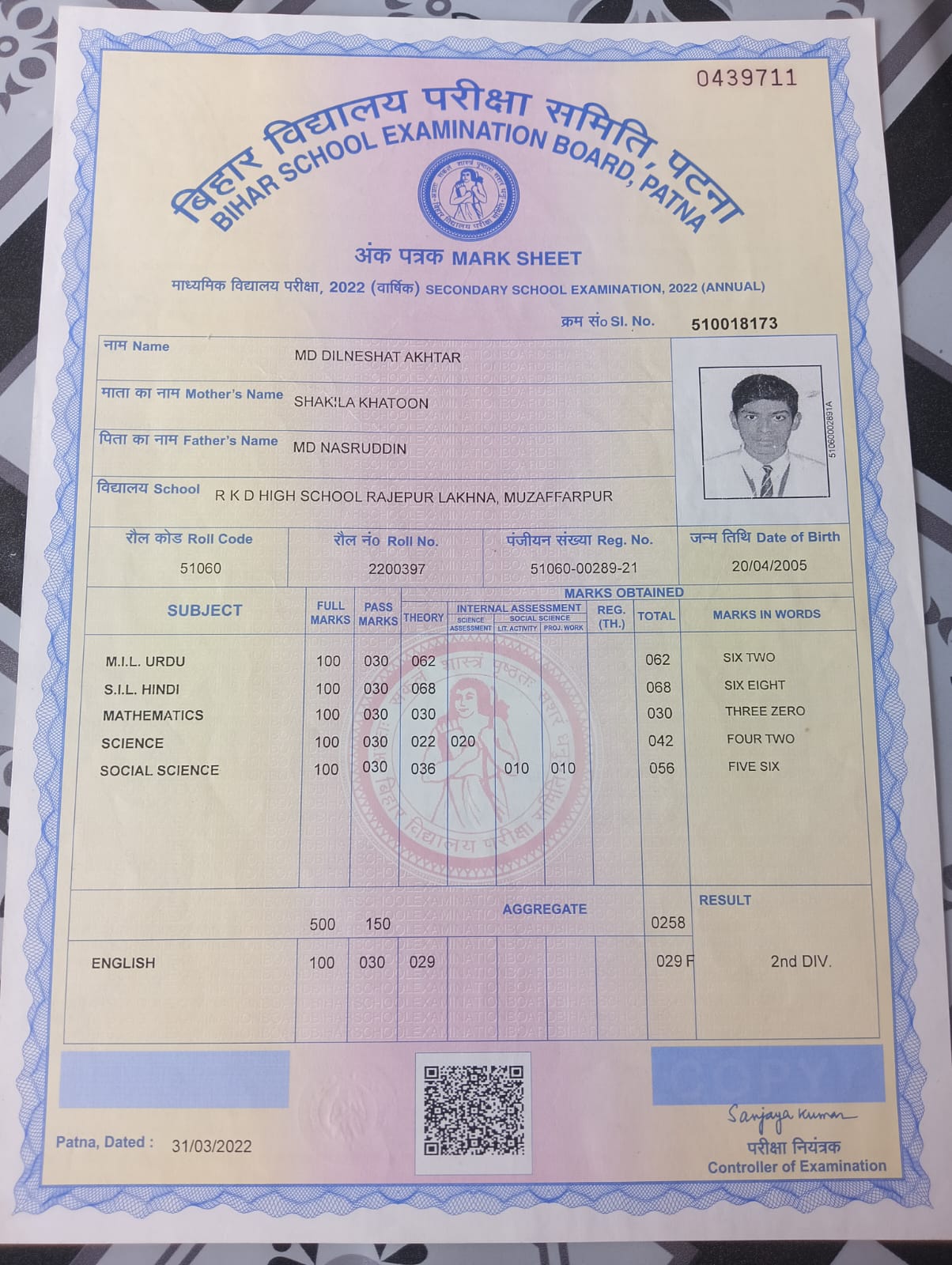
Marksheet
Correction Form
Duplicate Marksheet
Admission Form
Student Corner
Student Verification
Student Result
Contact Us
Course Detail
Home
Course Detail
Enroll Now
OPERATION THEATRE ASSISTANT
Add Student Detail
Branch Name*
--Select Branch--
Category Name*
--Select Category--
Sub Category Name*
--Select Sub Category--
Course Name*
--Select Course Name--
Session Name*
--Select Session Name--
Student Name*
Father Name*
Mother Name*
Dob*
Email*
Mobile*
Student Image(Max Size 80 KB)*
Your Recent Passpost Size Photo
Address*
State*
--Select State Name--
District Name*
--Select District Name--
City Name*
--Select City Name--
Category*
--Select Category Name--
Gender*
--Select Gender Type--
Male
Female
Other
Aadhar Card Number*
Document Image(Max Size 100 KB)*
10th Marksheet (DMC)